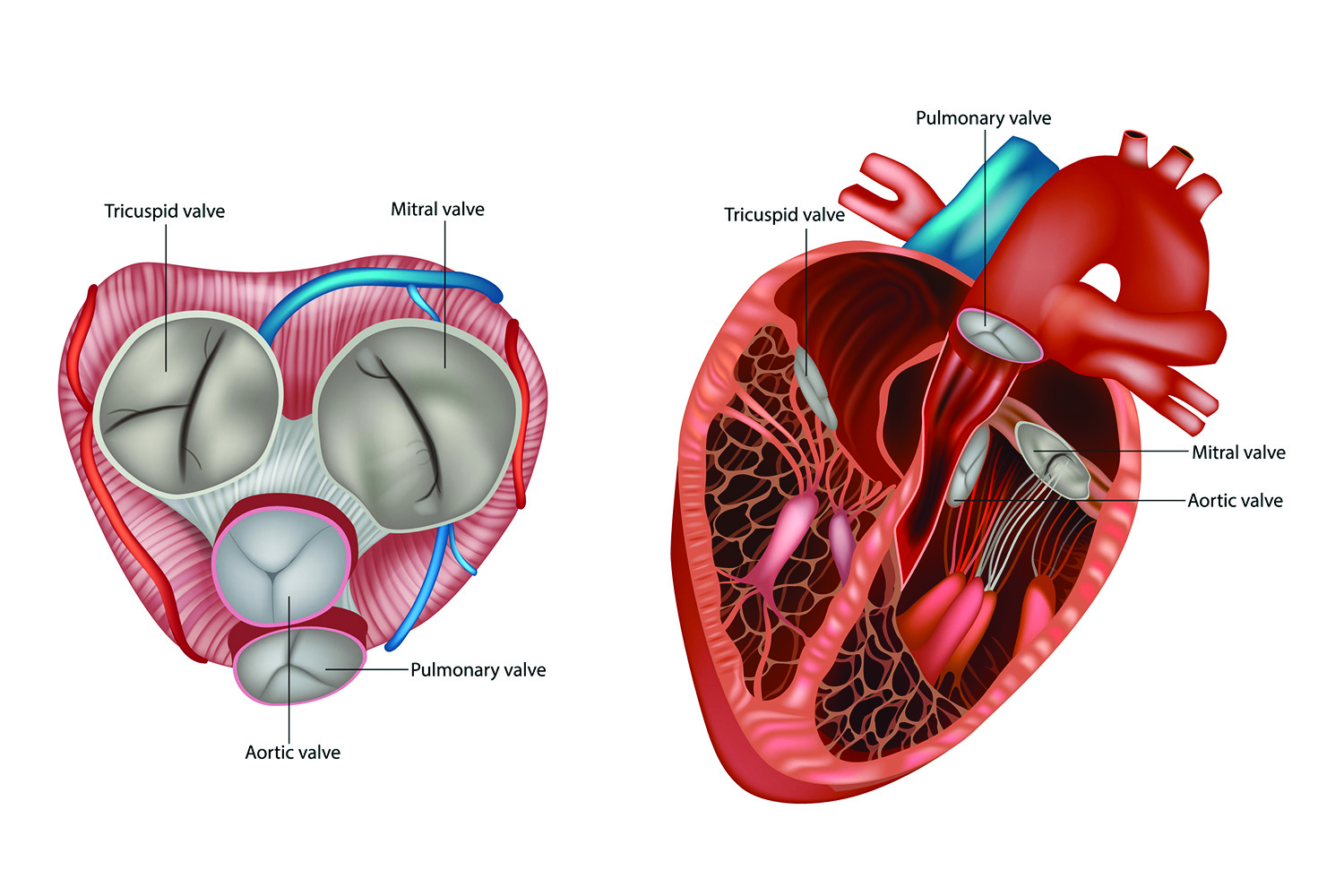
The heart has four valves that help control the direction of blood flow. One of these is the mitral valve, which sits between the left atrium and left ventricle. Oxygenated blood flows from the lungs into the left atrium. When the left atrium contracts, the mitral valve opens, directing blood into the left ventricle. When the left atrium relaxes, the mitral valve closes.
If the two flaps (leaflets) of the mitral valve fail to close tightly, blood can leak backward into the left atrium. This phenomenon is known as mitral regurgitation, and it forces the heart to work harder to meet the body’s need for oxygenated blood. Over time, the extra effort can cause the left ventricle to enlarge and thicken, leading to heart failure or other complications.
“If you have severe mitral regurgitation, we advise you to get the valve fixed,” says Marc Gillinov, MD, a Cleveland Clinic cardiac surgeon. “If you don’t, it will shorten your life.”
A leaky mitral valve can be repaired or replaced. Today, repair is favored over replacement, but replacement remains an excellent option.
Causes of Mitral Regurgitation
There are two types of mitral regurgitation:
- Primary mitral regurgitation is caused by the valve itself. The most common problem is mitral valve prolapse, a condition in which the valve leaflets become too floppy to shut properly. Rheumatic heart disease also can cause the mitral valve to leak, but because the leaflets become too stiff to shut properly.
- Secondary mitral regurgitation occurs when a disease of the heart muscle (ischemic, dilated or hypertrophic cardiomyopathy) or atrial fibrillation causes the heart to enlarge or change shape, distorting the valve and preventing its leaflets from closing normally.
Symptoms and Warning Signs
Mitral regurgitation often develops slowly. Individuals may have no symptoms or only mild symptoms for many years. However, in some individuals, mitral regurgitation develops quickly, causing severe symptoms to appear suddenly.
With either type of mitral regurgitation, the most common symptom is shortness of breath. Other symptoms may include:
- Persistent fatigue and lack of stamina
- Chronic cough
- Fast, pounding or fluttering heartbeat (palpitations)
- Feeling lightheaded without actually fainting
- Swollen feet or ankles
You also may experience atypical chest pain. Unlike the chest discomfort caused by a heart attack, atypical chest pain:
- May last for only a few seconds, then disappear
- Is a sharp or stabbing sensation
- May feel worse when you lie down
- Is not caused by exercise or relieved by rest
If you develop any of these symptoms, tell your primary care physician or a cardiologist.
However, if any of the following symptoms of acute mitral regurgitation occur suddenly, call 911:
- Breathing heavily, but feeling like you will suffocate
- Struggling to breathe while lying down
- Feeling tightness in your chest
How Mitral Regurgitation Is Diagnosed
Your doctor will start by reviewing your medical history and performing a physical exam that includes listening for a particular sound, called a heart murmur, with a stethoscope. If the results confirm mitral regurgitation, you will need to see a cardiologist for further testing.
A transthoracic echocardiogram is usually done to see how well your mitral valve is working. The test is painless and noninvasive and is often done in the doctor’s office. If a closer look at the valve is needed, a transesophageal echocardiogram may be ordered. This test requires sedation and may be done in a hospital or outpatient treatment center. Both tests are read by cardiologists.
Other tests may be needed to plan your treatment. They may include a cardiac computed tomography (CT) scan, magnetic resonance imaging (MRI) scan, exercise stress echocardiogram or cardiac catheterization.
Complications to Watch For
If mitral regurgitation is left untreated or is treated late, complications can develop.
Heart failure is the most common complication. Repairing or replacing the valve before symptoms appear can prevent heart failure from developing. If the valve is repaired or replaced after heart failure has begun, it may stop the condition from worsening and even reverse heart failure in many people.
Pulmonary hypertension can result when mitral regurgitation causes blood to back up, overloading the heart and raising blood pressure in the arteries that carry blood from the heart to the lungs.
The turbulent blood flow produced by mitral regurgitation can injure valve tissue, inviting bacteria to adhere and grow on the leaflets—a serious condition known as infective endocarditis.
Over time, chronic overload causes the heart to enlarge, stretching its electrical system and causing it to deliver inappropriate electrical signals. Chaotic electrical activity can produce atrial fibrillation, a major risk factor for stroke. Premature contractions can cause ventricular arrhythmias, which can be lethal.
“Mitral valves should be repaired as soon as severe regurgitation is recognized, even if you have no symptoms,” Dr. Gillinov says. “If you wait until your heart sustains damage, the likelihood of a normal life expectancy after valve repair drops.”
Treatment Options
A leaky mitral valve may be repaired or replaced. The best treatment for you will depend on whether your mitral regurgitation is primary or secondary and how severe it is, your age, and whether you have any conditions that increase the risk of complications.
“When repair is possible, it is the best option for severely prolapsed mitral valves,” Dr. Gillinov says. “Repair offers many advantages: It restores a normal life expectancy, avoids the need for blood thinners required with a mechanical valve replacement, and is likely to last longer than a bioprosthetic (pig or cow) valve replacement.”
Durability is desirable, because the average age of an individual undergoing mitral valve repair is 59. Today, 90% of repairs last 20 years: About 10% of individuals develop mitral regurgitation within 10 years and require another repair. Cleveland Clinic surgeons re-repair 70% to 80% of failed first repairs. When repair is not possible due to rheumatic heart disease, endocarditis, or heavily calcified leaflets, the valve is replaced.
Prolapsed mitral valves are most often repaired surgically, and 70% of isolated mitral valve repairs can be performed minimally invasively using a surgical robot. Robotic-assisted repairs use very small incisions, require shorter hospital stays, and allow a quicker return to normal activities.
Individuals who are not surgical candidates can undergo a nonsurgical approach called transcatheter edge-to-edge repair (TEER). The TEER procedure is performed by a cardiologist in a specially equipped cardiac procedure room. TEER is approved for patients who cannot undergo surgery, but the technique is being studied in lower-risk patients.
Lifestyle Adjustments
After mitral valve repair or replacement, you will need regular checkups and follow-up testing to ensure that your valve continues to work as it should. Be sure to comply with the schedule your cardiologist recommends.
To minimize the risk that regurgitation will recur, live a heart-healthy lifestyle. This means:
- Getting regular physical activity (including completing cardiac rehabilitation, if your cardiologist recommends it)
- Eating a healthy diet with lots of fruits, vegetables and healthy sources of protein
- Maintaining a normal weight
- Avoiding tobacco
- Minimizing stress
- Managing your blood pressure, blood sugar and cholesterol.
