For years, physicians could offer people with Alzheimer’s disease (Alzheimer’s disease) only medications to help enhance cognition and daily functioning. But while these drugs eased some symptoms, the underlying Alzheimer’s disease pathology continued to advance.
Today, two Alzheimer’s disease medications—donanemab (Kisunla) and lecanemab (Leqembi)—are changing the treatment paradigm. Recent research and growing real-world experience suggest these drugs not only alter the disease process but also may slow cognitive decline in people with early Alzheimer’s disease or mild cognitive impairment (MCI).
“For decades, there was a therapeutic nihilism about Alzheimer’s treatment in that you could give drugs for symptoms, but it really wouldn’t make a difference in the disease process,” says Charles Bernick, MD, with Cleveland Clinic’s Lou Ruvo Center for Brain Health. “If anything, these drugs provide some hope. In my 40 years in the field of Alzheimer’s disease, these are probably the most important therapeutic advances we’ve had.”
Starting treatment as early as possible is crucial, Dr. Bernick says. So, if you have cognitive troubles that concern you or your loved ones, mention them to your health-care provider, and discuss newly available blood tests that can help determine whether you’re a candidate for a new Alzheimer’s drug.
About the Alzheimer’s Disease Medications
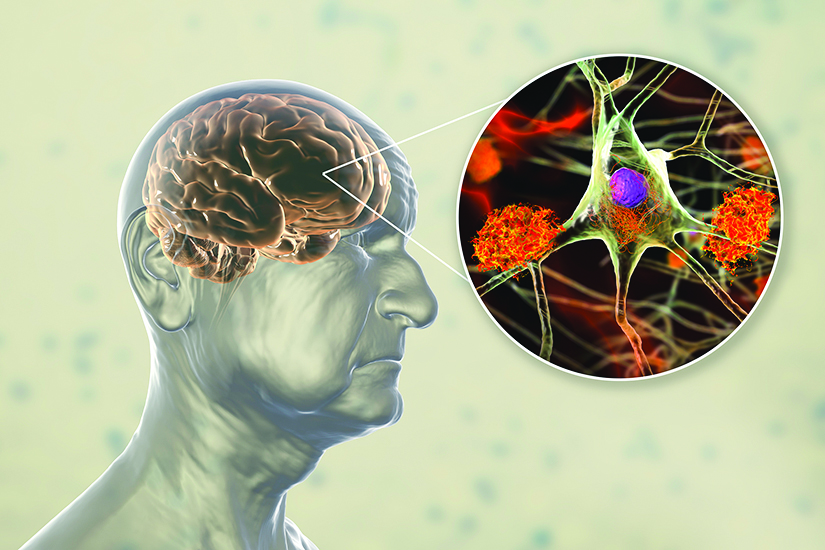
A hallmark sign of Alzheimer’s disease is the accumulation of the protein amyloid beta into plaques that interfere with communication between nerve cells (neurons) in the brain. In another component of the Alzheimer’s disease process, the protein tau forms twisted fibers, or neurofibrillary tangles, within the neurons.
Known as antiamyloid monoclonal antibodies, the two Alzheimer’s disease medications clear amyloid beta from the brain and, in doing so, may also slow tau propagation. In clinical trials, both drugs reduced amyloid plaque burden and slowed cognitive decline in people with early Alzheimer’s disease or MCI over 18 months.
And, researchers from Yale University School of Medicine, Harvard Medical School, and other institutions reported results of an extension study showing that the benefits produced by lecanemab continued to accrue for up to 36 months. The participants with lower amyloid burden generally stabilized or improved from 18 to 36 months, supporting early initiation of treatment, the study authors wrote (Alzheimer’s & Dementia, December 2025).
“With the initial studies, we’re talking an 18-month period,” Dr. Bernick says. “But we know from following individuals over two to three years that there’s a suggestion that the effect continues to increase—that is, the longer you’re on the drug, the more benefits you’re going to get in changing the trajectory of the disease. Of course, that doesn’t necessarily mean people will improve, but it is slowing progression.”
- Donanemab and lecanemab are indicated for people with symptoms of early Alzheimer’s disease or MCI who have evidence of Alzheimer’s disease-related pathology in the brain.
- The drugs are not a “cure” for Alzheimer’s disease, but they have been shown to slow disease progression and cognitive decline.
- Medicare covers the cost of the drugs and the necessary testing, but coverage among private insurers may vary. Check to see what your provider covers.
What to Expect from Donanemab and Lecanemab
Both drugs are administered by intravenous infusion—monthly for donanemab and every two weeks for lecanemab. After 18 months of lecanemab treatment, patients may continue with monthly infusions or switch to a recently available self-injected form, administered once a week. With donanemab, the drug may be stopped if imaging studies show sufficient amyloid plaque clearance from the brain, although the degree to which the clinical benefits of the drug are maintained after stopping therapy remains unclear. Typically, the antiamyloid drugs are combined with cognition enhancers, such as donepezil (Adlarity, Aricept), galantamine (Razadyne, Reminyl), rivastigmine (Exelon), and memantine (Namenda).
As of early 2026, over 180 patients at the Lou Ruvo Center for Brain Health were being treated with donanemab or lecanemab, and patients and their families have largely been satisfied with them, Dr. Bernick says. Yet, while the drugs have demonstrated efficacy in study populations, he acknowledges the challenges of gauging their effects on an individual level.
“The problem is you can’t know how someone would have been without the drugs,” Dr. Bernick says. “We tell patients, ‘You almost have to take it on faith, based on all the studies, that these drugs will slow your decline.’”
Antiamyloid drugs are associated with a greater risk of amyloid-related imaging abnormalities (ARIAs), which can present as swelling or bleeding in the brain and, less commonly, manifest as potentially life-threatening brain bleeding and fluid accumulation. Individuals with the APOE4 gene have the greatest risk of this complication, so you should be tested for it before starting treatment and undergo imaging studies to monitor for ARIAs before and during treatment.
Fortunately, Dr. Bernick notes that he and his colleagues have not witnessed these serious adverse events among their patients: “If you choose the correct patient and if you’re careful about the monitoring, these drugs can be administered safely.”
Alzheimer’s Blood Tests
Alzheimer’s disease can be confirmed using amyloid positron emission tomography (PET) imaging scans or a lumbar puncture to analyze cerebrospinal fluid. Although effective, these tools are expensive, not readily available to everyone and, in the case of lumbar puncture, invasive.
Now, if Alzheimer’s disease is suspected, two blood tests can measure levels of amyloid beta and phosphorylated tau to help determine eligibility for antiamyloid therapy. The tests, available by prescription, are indicated only for people ages 55 and older. Depending on the test results, PET imaging or a CSF analysis is necessary to confirm treatment eligibility.
If you have cognitive complaints, have your doctor administer a basic dementia screening test. Then, if warranted, your physician may order a blood test or refer you to a specialist for further evaluation.
Overall, Dr. Bernick says the new Alzheimer’s disease medications, coupled with the new blood tests, mark an important step in the journey toward a new, more effective way to manage Alzheimer’s disease.
“To me, the biggest thing is making people aware that these drugs and tests are available,” he says. “There is a big push to get people identified earlier and then given at least the option of treatment. Clearly, you’d rather do an antiamyloid treatment the earlier you can. I think it’s very optimistic for the future that we will have strategies that can truly change the course of this whole disease process.”
- Forgetting recently learned information
- Problems remembering to pay bills or managing your finances
- Difficulty focusing; losing your train of thought
- Getting lost in familiar places; forgetting where you are or how you got there
- Repeating yourself more frequently within a shorter period of time
- Inability to follow directions; trouble following a familiar recipe
- Failing to recognize familiar people
- Forgetting to take your medications as prescribed
- Difficulty following/joining conversations or understanding verbal or written words
- Forgetting where things belong; putting things in unusual places
- Withdrawing from social situations due to problems with holding a conversation
- Trouble maintaining personal hygiene
- Mood changes (e.g., becoming more irritable, suspicious, anxious, easily upset)
Source: Alzheimer’s Association
