If you have been told you have the bone-thinning disease osteoporosis, your doctor probably will recommend you adopt lifestyle strategies that may help boost your bone strength and prevent fractures in older age.
These strategies include consuming plenty of calcium-rich foods, making sure you get enough vitamin D, and getting plenty of weight-bearing exercise (e.g., walking, running, lifting weights). Dietary calcium is deposited in bones, where it binds with other minerals to strengthen bone, while vitamin D helps improve the body’s absorption of calcium from food. Weight-bearing exercises are helpful because they subject the bones to stress that stimulates the formation of new bone.
Osteoporosis medications also are effective at preserving bone strength and decreasing the risk of fractures. Phoebe Ke, PA-C, MHA, CCD, a clinically advanced physician assistant in Mount Sinai’s Department of Orthopedics, explains how these drugs work.
Osteoporosis Medications
|
ANTIRESORPTIVE DRUGS |
||
| Drug Class | Drug Name | Possible Side Effects |
| Bisphosphonates | Alendronate (Fosamax, Binosto); ibandronate (Boniva; risedronate (Actonel, Atelvia); zoledronic acid (Reclast) | Muscle pain; esophagitis; osteonecrosis of the jaw; atypical fractures of the femur |
| SERM | Raloxifene (Evista) | Joint pain; hot flashes during first six months of treatment; blood clots; stroke |
| Monoclonal antibody | Denosumab (Prolia) | Osteonecrosis of the jaw; atypical fractures of the femur; low blood calcium; weakened immune system |
|
ANABOLIC BONE DRUGS |
||
| Drug Class | Drug Name | Possible Side Effects |
| Parathyroid Hormone/PTHrP | Teriparatide (Forteo), abaloparatide (Tymlos) | Muscle pain; increased blood calcium; postural hypotension; kidney stones |
| Monoclonal Antibody | Romosozumab (Evenity) | Hypocalcemia; heart attack; stroke |
Fosamax, Prolia and Other Antiresorptive Drugs
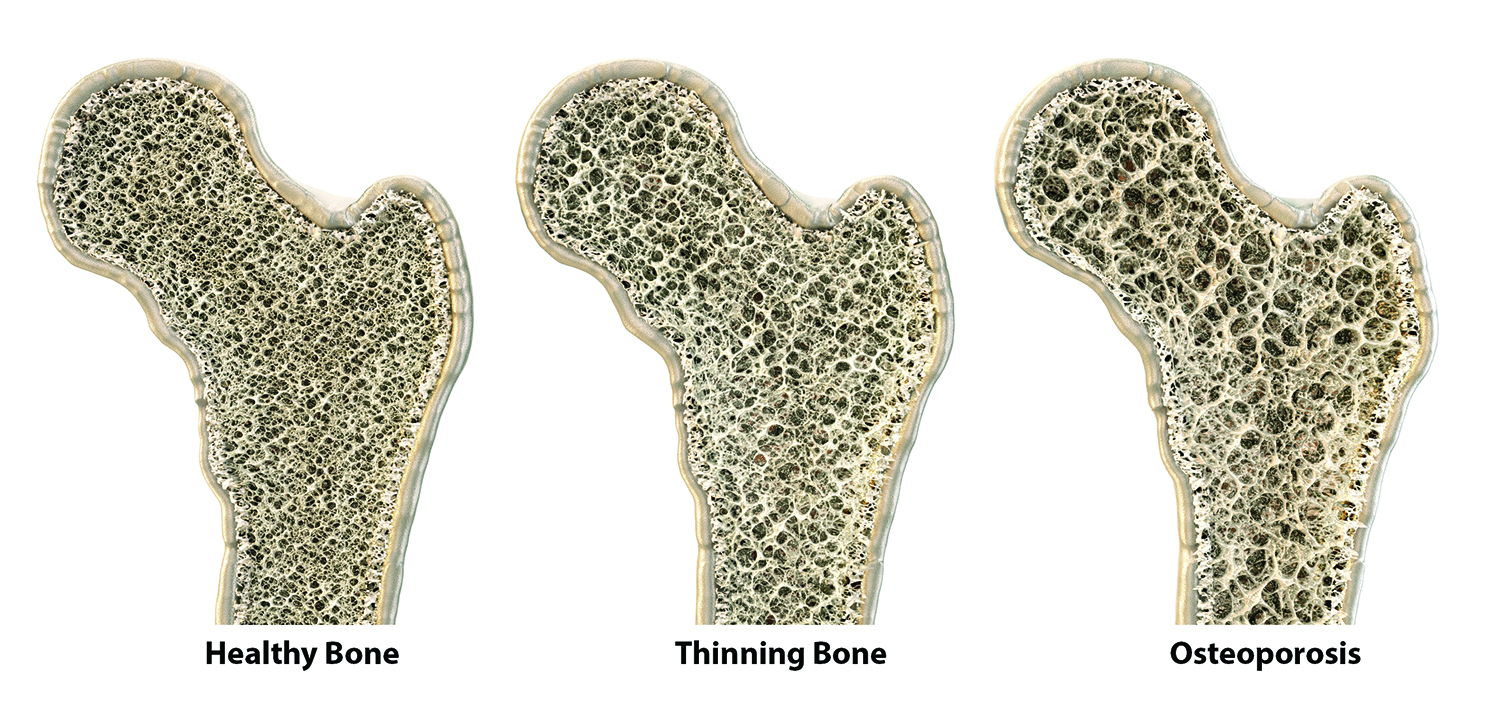
Even though your bones may seem inert, they undergo a constant process of bone breakdown and formation, called remodeling.
“Put simply, old bone is broken down by cells called osteoclasts, and new bone is formed by cells called osteoblasts,” Ke says. “In younger people, bone breakdown is balanced by bone building, but in older adults, this balance is lost—more old bone is broken down and less new bone is created, leaving bones less dense. This is what we know as osteoporosis, and it makes people more vulnerable to fractures.”
Antiresorptive osteoporosis medications interfere with bone breakdown. Alendronate (Fosamax, Binosto) and other bisphosphonate drugs are among these types of medications.
“The most commonly used antiresorptives are bisphosphonates,” Ke notes. “The drugs usually are given as a once-daily or once-weekly oral pill, but there also are more potent bisphosphonates that can be given annually via intravenous infusion if indicated. These typically are reserved for people who are at particularly high risk for fracture.”
Women with osteoporosis who are at high risk of breast cancer may benefit from taking a selective estrogen receptor modulator (SERM). These drugs, which come in daily pill form, mimic the effects of estrogen on bone. “Estrogen plays a major role in balancing bone breakdown and creation, but after menopause levels of the hormone drop substantially,” Ke says. “This is one reason why older women are at greater risk of osteoporosis than older men.”
Another type of antiresorptive, denosumab (Prolia), is given by injection every six months. It may be prescribed in place of bisphosphonates for people with osteoporosis who also have mild-to-moderate chronic kidney disease (CKD), since bisphosphonates are excreted by the kidneys and this can cause issues if kidney function is impaired. Denosumab is a monoclonal antibody. The latter mimic proteins that are naturally produced by the immune system and can be used to neutralize other proteins. In the case of denosumab, the target protein is RANK ligand (RANK-L), which stimulates the formation and survival of the osteoclasts that otherwise would resorb bone.
Anabolic Osteoporosis Medications
Anabolic drugs aid bone formation and typically are prescribed to people with worsening osteoporosis and those who are at particularly high risk of sustaining a fracture. Examples include synthetic versions of parathyroid hormone and parathyroid hormone-related protein (PTHrP), which are given by daily injection. Both help regulate calcium levels in the bloodstream, but their primary purpose is to stimulate osteoblasts to create bone. A newer anabolic drug—a type of monoclonal antibody called romosozumab (Evenity)—is given as a monthly injection and targets an immune system protein that otherwise would inhibit the action of osteoblasts.
Side Effects of Osteoporosis Medications
Osteoporosis drug side effects range from relatively minor to potentially harmful. For example, oral bisphosphonates may cause gastrointestinal (GI) issues, and they also raise the risk of esophagitis (inflammation of the esophagus), which can be so painful it affects your ability to eat (to help prevent this side effect, take the drugs before you eat and stay upright for the next 30 minutes). Intravenous bisphosphonates do not have the same GI-related side effects but can cause transient flu-like symptoms, musculoskeletal pain, excessively low calcium levels—known as hypocalcemia—and kidney injury.
Both oral and intravenous bisphosphonates are associated with an increased risk of osteonecrosis of the jaw (an infection of the jawbone), particularly in people who have cancer and are taking higher doses of their bone drugs and those taking steroids or immunosuppressive drugs. “Atypical” fractures of the femur (thigh bone) also are a risk for people taking both formulations of bisphosphonate, as well as for those taking denosumab. These side effects are rare, but it is wise to stay alert for symptoms that may indicate a problem. Atypical fractures may be preceded by groin or thigh pain for several weeks, while osteonecrosis of the jaw causes gum pain and swelling, loose teeth, and numbness in the jaw.
Denosumab also increases the risk of skin infections in people who have a weak immune system or take immunosuppressant drugs. Signs of infection may include fever, chills, red and swollen skin, and skin that feels hot. And, while denosumab often is prescribed to people with impaired kidney function, it may not be suitable for people with advanced CKD and those undergoing kidney dialysis, since it can cause hypocalcemia in these individuals. The same hypocalcemia risk applies to romosozumab, and the latter also raises the risk of serious cardiovascular events like heart attack and stroke. The U.S. Food & Drug Administration approved the drug for a treatment duration of one year.
SERMs may raise the risk of deep vein thrombosis (DVT: a blood clot in one of the deep veins of the leg or arm), so both are contraindicated in women who have a history of stroke, or who have very high blood pressure and/or the abnormal heart rhythm atrial fibrillation (both stroke risk factors). Signs of a possible DVT include swelling, warmth and pain in the legs. Parathyroid hormone analogs and PTHrP analogs may cause postural hypotension (low blood pressure when changing position; for example, when you stand up from sitting down). This can cause fainting that may result in injury.
Benefits and Risks of Osteoporosis Medications
Serious side effects from osteoporosis medications are extremely rare. However, hip fractures are common in older adults with osteoporosis and can result in disability and death. For this reason, the benefits of osteoporosis drugs favor use of the medications if you have osteoporosis, and your health-care provider will take precautions to help you stay safe if you are using these drugs. For example, you probably will undergo periodic bone density testing to check if the drugs are still necessary, and people who take denosumab or romosozumab will have their calcium levels checked before each dose.
“People taking bisphosphonates are advised to take a break from the drugs after three to five years,” Ke says. “The medication builds up in your bones, so when you stop taking the drugs their positive effects persist, though you may need to start taking them again if your bone density declines. Denosumab can be safely administered for 10 years—the specific duration is up to the provider and patient to decide.”
People who take parathyroid hormone analogs or PTHrP are advised to discontinue these after two years, though exceptions may be made for people whose fracture risk remains high.
