Hidradenitis suppurativa can be an unpredictable disease. One person may have an occasional small, painful bump in the armpit, while another may have chronic pain, severe scarring, and inflammatory bowel disease. But there is one thing that many people with HS have in common: a long, frustrating road filled with misdiagnoses and failed treatments. On average, it takes seven to 10 years after symptoms appear to get an HS diagnosis, researchers reported in the journal Dermatology. That delay can be devastating: Untreated, this chronic inflammatory condition can worsen, causing severe pain, scarring, odor, and disability.
Understanding HS
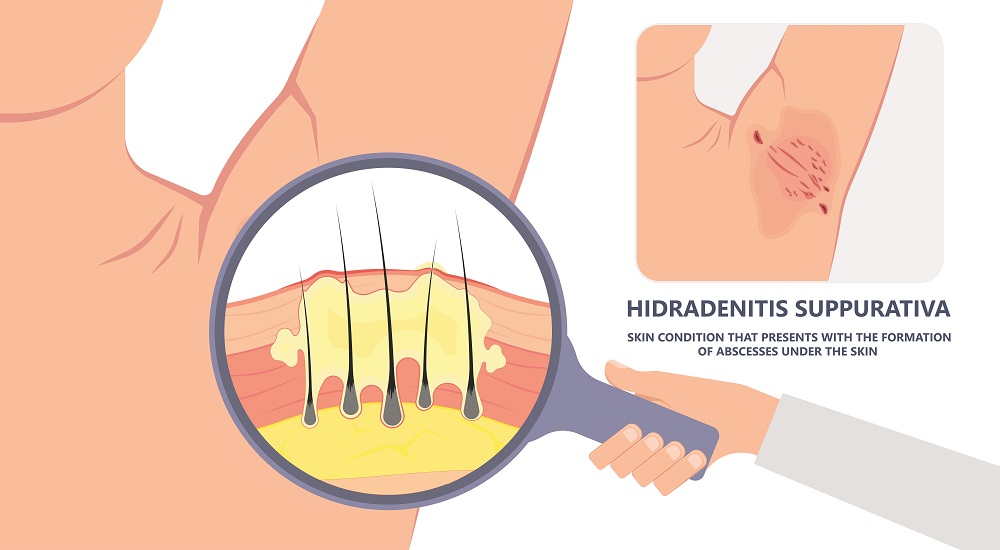
HS begins when a hair follicle becomes blocked and forms a small, painful bump. It most often strikes in areas with apocrine sweat glands—such as the armpits and the groin—as well as under and around the breasts. It can progress through three stages (see table) and can become severe enough to interfere with normal functioning and movement, even causing disability.
People with HS also have a higher risk of a variety of other conditions, including diabetes, squamous cell carcinoma, obesity, metabolic disorders, spondyloarthritis, PAPA syndrome (pyogenic arthritis, pyoderma gangrenosum and acne), polycystic ovarian syndrome, hypertension, dyslipidemia, inflammatory bowel disease, and spondyloarthropathy.
Prevention and treatment
While there is no cure for HS, early diagnosis and treatment can limit inflammation and skin damage, and lower the risk of systemic conditions. Management takes a multipronged approach:
Lose weight if necessary. While HS strikes people of any body weight, it is more prevalent among people with obesity. While the relationship is complicated—obesity may occur with HS but not cause it—researchers in Denmark found that the number of patients reporting HS symptoms after weight loss from bariatric surgery decreased by 35 percent. They concluded that a weight loss of more than 15 percent was associated with a significant reduction in disease severity.
Don’t smoke. Researchers recently discovered that deficiency in a cell-communication system called the Notch pathway likely plays a causal role in HS. Smoking suppresses Notch signaling, which is why smokers with HS have more affected body areas than nonsmokers.
Use antibacterial washes. HS nodules are highly prone to infections. To reduce the risk, use antimicrobial washes such as chlorhexidine (Peridex, Hibiclens) or benzoyl peroxide (an ingredient in a wide variety of anti-acne products). Some dermatologists recommend bleach baths, where you soak in a 0.005% diluted bleach solution for five to 10 minutes twice per week. (Never put full-strength bleach on your skin.)
Lifestyle. Avoid irritating your skin by keeping high-risk areas cool and dry, wearing loose-fitting clothing, and replacing shaving with clippers, waxing, or laser hair removal.
In-office procedures
Depending on your specific condition, your dermatologist may suggest an in-office procedure to address the nodules or abscesses:
- Steroid injections can reduce inflammation and the size of non-infected nodules.
- Abscesses can be drained in the office, but there is a high rate of recurrence.
- Your dermatologist or a plastic surgeon may “deroof” an abscess by removing the skin that covers it or may excise the whole lesion and any tunnel.
- Laser surgery can help treat lesions and scars in some patients whose disease is otherwise stable and medically managed.
- Laser hair removal can prevent outbreaks by destroying the hair follicles in high-risk areas.
While these procedures can address the disease in a particular location, they don’t prevent flares from appearing on other parts of the body or address underlying inflammation, so medical management is important even when these are successful.
Medications for HS
A variety of medications show promise in managing HS:
Creams. Topical antibiotics such as clindamycin (Cleocin T, Clindagel) and dapsone (Aczone) can help treat infection and reduce inflammation. A topical corticosteroid such as triamcinolone (Cinolar, Kenalog, Triderm) can reduce local inflammation, but it should be used only for short periods of time (up to two weeks) to avoid damaging the skin. Topical resorcinol (Resinol, R A Acne) can open clogged hair follicles and reduce inflammation.
Oral antibiotics. A class of drugs called tetracyclines have both antibacterial and anti-inflammatory properties. A common first choice is doxycycline (Vibramycin, Doryx, Oracea, Acticlate, Atridox, Doxy). This medication can cause severe nausea, so let your doctor know if you need to try a different drug.
Hormonal medications. HS strikes follicles with associated apocrine glands. Apocrine glands are inactive until hormonal changes at puberty. Drugs that block the effects of androgens such as testosterone help many people with HS.
These include spironolactone (Aldactone) and finasteride (Proscar, Propecia). Birth control pills can also help women who have menstrual-related flares.
Metformin (Glucophage), which is commonly used to treat diabetes, can reduce HS-related inflammation. One small study found that about 70 percent of people who took metformin had improvement in their symptoms and quality of life.
Biologics. For moderate to severe disease, biologic medications are very promising. In fact, the only medication specifically approved to treat HS is adalimumab (Humira). Studies show that people who received adalimumab injections have “noticeably fewer abscesses (lumps with pus) and nodules (hard, deep lumps),” the American Academy of Dermatology reports.
Access to quality care
Not all dermatologists treat HS, so you may need to shop around. Look for a board-certified dermatologist who is familiar with the latest advances in HS. (Doctors who have more recently completed medical school may be more up-to-date on the latest advances in treating this disease.)
